
Fractures — or broken bones — are among the most common injuries seen in children and adolescents. A child’s skeleton is fundamentally different from an adult’s: it is more porous, more flexible, and still actively growing. These properties mean that children’s fractures often behave differently, heal more quickly, and carry a much better long-term prognosis than equivalent injuries in adults. Understanding how fractures are assessed and treated can help parents make sense of what can otherwise feel like an overwhelming experience.
At Dr. Bansal’s Arogya Hospital, Dr. Ankita Bansal and Dr. Vijay Bansal believe that no two fractures are alike. Treatment is always individualised — tailored to the child’s age, the nature of the injury, and their specific growth trajectory — rather than following a one-size-fits-all protocol. This blog walks through the key principles that guide fracture management in children, so parents and referring physicians can better understand the reasoning behind each treatment decision. For a detailed discussion of specific fracture types, please refer to our blog on Types of Fractures in Children. Growth plate injuries are covered separately in our blog on Growth Plate Injuries.
What Determines How a Fracture Is Treated?
When evaluating a child’s fracture, several key variables are considered together to determine the most appropriate course of treatment. Each child is assessed individually, and the treatment plan is customised accordingly.
1. Age of the Child
A child’s age is one of the most significant factors in treatment planning. Younger children have a greater amount of skeletal growth remaining, which gives their bones a remarkable capacity to heal and remodel — that is, to gradually return to a normal shape even if the initial alignment is not perfect. As a result, younger children can often be managed successfully with a cast alone, whereas older children and adolescents, whose growth is nearly complete, may require surgical stabilisation to achieve and maintain acceptable alignment.
This does not mean that older children face worse outcomes — simply that the threshold for surgical intervention is lower as the child approaches skeletal maturity, because the natural corrective potential of growth is diminishing.
2. Fracture Location
Where on the bone the fracture has occurred matters enormously. Fractures near the ends of long bones, particularly those involving the growth plate (physis), are managed with particular care. Fractures in the shaft of a bone may be more forgiving, while those involving a joint surface require precise reduction to prevent long-term stiffness or arthritis. The blood supply to the bone at a given location also influences how readily it heals.
3. Displacement and Angulation
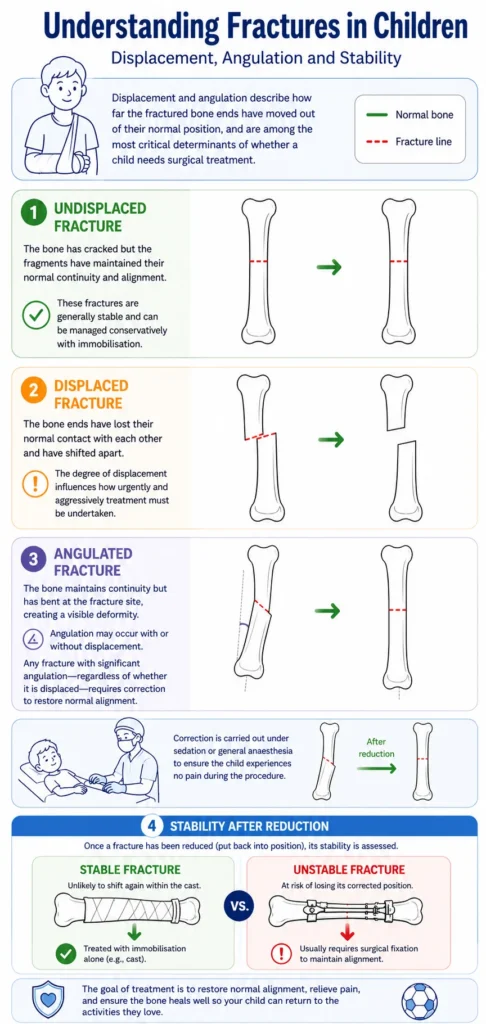
Displacement and angulation describe how far the fractured bone ends have moved out of their normal position, and are among the most critical determinants of whether a child needs surgical treatment.
An undisplaced fracture is one where the bone has cracked but the fragments have maintained their normal continuity and alignment. These fractures are generally stable and can be managed conservatively with immobilisation.
A displaced fracture is one where the bone ends have lost their normal contact with each other and have shifted apart. The degree of displacement influences how urgently and aggressively treatment must be undertaken.
An angulated fracture is one where the bone maintains continuity but has bent at the fracture site, creating a visible deformity. Angulation may occur with or without displacement. Any fracture with significant angulation — regardless of whether it is displaced — requires correction to restore normal alignment. This is carried out under sedation or general anaesthesia to ensure the child experiences no pain during the procedure.
Once a fracture has been reduced (put back into position), its stability is assessed. A stable fracture — one that is unlikely to shift again within the cast — may be treated with immobilisation alone. An unstable fracture is at risk of losing its corrected position, and will usually require surgical fixation.
4. Type of Fracture
The pattern of a fracture provides important information about its stability and the likely treatment required. As discussed in detail in our fractures types blog, common patterns in children include torus (buckle) fractures, greenstick fractures, hairline (stress) fractures, and plastic deformation, each with its own management pathway. In brief:
- Torus and hairline fractures are generally stable and heal well with short-term immobilisation alone, without the need for surgery.
- Greenstick fractures, especially those with significant angulation, often require manipulation under anaesthesia to correct the bend before casting.
- Plastic deformation — where the bone has bent without a clear fracture line — similarly requires correction under anaesthesia when the deformity is functionally significant.
- Growth plate injuries are assessed individually based on their classification and degree of displacement, and are covered in detail in our dedicated blog on this topic.
Treatment Procedures
Treatment of a paediatric fracture begins, wherever possible, with an attempt at closed reduction — correcting the alignment of the bone without making a surgical incision. This is performed under general anaesthesia or conscious sedation, ensuring the child is comfortable throughout. Once the fracture is reduced, the surgeon assesses the stability of the reduction and determines whether a cast alone will suffice, or whether additional fixation is required.
Closed Reduction and Casting
For many fractures, particularly those in younger children or those that are inherently stable after reduction, a well-moulded plaster or fibreglass cast provides sufficient immobilisation for healing to occur. The cast holds the bone in its corrected position while the body lays down new bone bridging the fracture site. The duration of casting varies depending on the bone involved, the child’s age, and the nature of the fracture, but typically ranges from three to six weeks.

Surgical Stabilisation
When a fracture is deemed unstable — at high risk of shifting within the cast — or when closed reduction alone cannot achieve adequate alignment, surgical stabilisation is required. The goal is to hold the fracture in its corrected position while healing occurs. Treatment is customised to each child based on the fracture pattern, bone involved, and age. A detailed discussion of the implants used is available in our companion blog on Common Implants Used in Paediatric Orthopaedics. The main surgical options include:
- Percutaneous fixation: Wires or screws are passed through the skin into the bone from a point away from the fracture site, stabilising the fracture without a formal open incision. Commonly used for supracondylar fractures of the humerus and certain wrist fractures.
- K-wire fixation: Kirschner wires (K-wires) are fine stainless steel pins used to hold fracture fragments in place, either after closed or open reduction. They are typically removed once healing is confirmed.

- Titanium Elastic Nailing (TENs): Flexible titanium nails are passed up the medullary canal of long bones, providing internal splintage while preserving the biology of healing. A popular and effective technique for forearm and femoral shaft fractures in children.

- Plate fixation: A metal plate is applied to the surface of the bone and secured with screws to provide rigid stabilisation. Used in more complex fractures or in older children approaching skeletal maturity.

- Intramedullary nailing: A rigid nail passed down the canal of the bone. Commonly used in adolescent femur fractures, where a stronger construct is required.
- Open reduction: When closed methods cannot achieve adequate reduction, the fracture site is surgically exposed to allow direct visualisation and precise realignment before fixation.
- External Fixation: Wires and rods are placed externally to align the bone to allow the fracture to heal. These are then removed once adequate fracture healing occurs.
 How Fractures Heal
How Fractures Heal
Fracture healing in children is a robust biological process. As the fracture repairs, the body produces new bone tissue — visible on X-ray as callus — which progressively bridges and stabilises the fracture site. The presence of adequate callus on follow-up X-rays is a reliable indicator that healing is progressing well. The rate of healing varies with the child’s age, the bone involved, and the nature of the fracture. For a detailed discussion of the stages of fracture healing, please refer to our blog on How Fractures Heal.
Remodelling: The Child’s Unique Advantage
One of the most remarkable features of the paediatric skeleton is its capacity for remodelling — a process by which a bone that has healed in a slightly imperfect position continues to reshape itself over time, progressively restoring a more normal contour. Remodelling is specific to growing children and does not occur to any meaningful degree in adults. The younger the child, the greater the remodelling potential. For a fuller explanation of this process, please refer to our blog on How Fractures Heal.
What Are ‘Acceptable Criteria’?
Parents frequently hear their child’s surgeon use the phrase ‘acceptable alignment’ or ‘within acceptable criteria.’ This can be confusing — if a bone is broken, why is it not put back perfectly straight? The answer lies in the principles of remodelling and the risks of intervention.
Acceptable criteria define the range of residual angulation or displacement that, based on the child’s age and the bone involved, is predicted to remodel satisfactorily without the need for surgical correction. These thresholds are not arbitrary — they are based on decades of clinical experience and outcome data. Fractures that fall within acceptable criteria are expected to heal with a normal functional result, even if the initial X-ray appearance is not perfect.
Crucially, acceptable criteria differ according to the child’s age and the specific bone and joint involved. A degree of angulation that is entirely acceptable in a six-year-old’s forearm may be unacceptable in a fifteen-year-old’s. At Dr. Bansal’s Arogya Hospital, each child’s fracture is assessed individually by Dr. Ankita Bansal and Dr. Vijay Bansal, and the treatment plan is tailored accordingly — ensuring that every decision is made with that child’s growth potential and long-term outcome in mind.
It is important to reassure parents that almost all children’s fractures heal. The vast majority go on to full functional recovery, often with surprisingly little residual evidence that a fracture ever occurred.
Conclusion
Managing fractures in children requires a nuanced understanding of the growing skeleton — its vulnerabilities, its healing capacity, and its remarkable ability to remodel. Treatment decisions are guided by the child’s age, the location and pattern of the fracture, and the degree of displacement or angulation present. Where possible, non-surgical management with closed reduction and casting is preferred. When fractures are unstable or irreducible by closed means, a range of surgical options — from percutaneous K-wire fixation to TENs nailing and plating — allow safe, reliable stabilisation while preserving the biology of healing.
At Dr. Bansal’s Arogya Hospital, we are committed to providing personalised, evidence-based care for every child. No two fractures are managed the same way — treatment is customised to each patient’s age, injury pattern, and individual needs, with the goal of achieving the best possible long-term outcome. Parents can be reassured that children’s bones heal remarkably well, and that with appropriate, tailored treatment, the overwhelming majority of paediatric fractures resolve with excellent functional results.