A guide for parents — what to expect from diagnosis to recovery
What are growth plates — and why do they matter?

At the ends of every growing bone in a child’s body lies a thin layer of cartilage called a growth plate — medically known as the physis. These structures are the engine of skeletal growth: new cartilage is continuously produced here and gradually converted into solid bone, allowing a child’s bones to grow longer over time.
Because growth plates are made of soft cartilage rather than hard bone, they are the weakest point in a child’s skeleton. A force that might cause a ligament sprain in an adult can fracture through the growth plate in a child. This is what makes childhood bone injuries unique — and why they need specialist attention.
Good to know: The active, well-supplied nature of growth plates also means fractures near them tend to heal faster than fractures in the middle of a bone. Children’s bones have remarkable healing potential.
What is a growth plate injury?
A growth plate injury — also called a physeal fracture — is a break in a bone that extends into or through the growth plate. These are among the most common fractures in children and teenagers.
No two growth plate injuries are the same. They vary by location in the body, the pattern of the break, how much the bone ends have shifted, and the child’s age. Each of these factors matters equally when deciding on the best treatment.
How is a growth plate injury diagnosed?

In most cases, plain X-rays are enough to identify a physeal fracture. However, because growth plate cartilage does not show up on X-rays, the growth plate appears as a normal gap in the bone — which can sometimes look similar to a fracture line.
For this reason, Dr. Ankita Bansal routinely requests X-rays of the opposite limb as well — to compare normal anatomy and spot subtle differences that might indicate injury on the affected side.
When the fracture is complex, or when it is important to check whether the break extends into the joint, a CT scan or MRI may be recommended. MRI is the only imaging that can show damage to the cartilage of the growth plate itself.
Initial treatment and approach
The moment your child arrives at Arogya Hospital, the first priority is relieving pain and protecting the injured limb. A posterior slab — a plaster splint applied to the back of the limb — is applied promptly. This controls pain, reduces swelling, and keeps the bones in position without encasing the whole limb, which is important in the early days when swelling is still settling.
This type of splint does not interfere with MRI or CT scans, and can be temporarily removed for X-ray review and then reapplied.
Definitive treatment depends on four equally important factors:
- Type of fracture — the Salter-Harris classification
- Displacement — how much the bone ends have shifted
- Location — which bone and growth plate is involved
- Age and growth remaining — how much growing the child has left to do
The goal of treatment is always to restore normal or near-normal alignment, preserve joint function, and minimise the risk of any long-term growth disturbance.
Do all growth plate injuries need surgery?
No — and in fact, the majority of growth plate injuries do not require surgery. Most children with these injuries are managed very successfully with a plaster cast alone.
Managed without surgery
Fractures where the bones are still well-aligned, or can be gently repositioned without an operation. A cast is applied and the child is monitored as the bone heals.
Surgery may be needed
Fractures where the bone has shifted significantly, the break enters the joint, or the bones cannot be held in place with a cast alone. Surgery uses wires or screws to hold everything in position while healing occurs.
Dr. Ankita Bansal’s approach: Surgery is only recommended when it is genuinely necessary to achieve good alignment and protect the growth plate. Every case is assessed individually, and the simplest effective treatment is always preferred.
What complications can occur?

Every child’s body responds differently to a growth plate injury. The amount of damage to the growth plate cartilage cannot always be assessed on X-rays at the time of injury — only an MRI can provide that detail, though this is not always needed for treatment decisions.
Possible long-term complications depend on the severity of injury, which growth plate is involved, how much the bone shifted, and how much growing the child still has to do. These include:
Growth arrest — the injured growth plate slows or stops producing new bone, causing that limb to become shorter than the other side.
Angular deformity — if only part of the growth plate is damaged, one side of the bone may continue growing while the other does not, causing the bone to curve or tilt.
Joint problems — fractures that disturb the joint surface can lead to stiffness or early arthritis if not restored to proper alignment.
Because these complications can appear months or even years after the original injury, children with significant growth plate fractures are monitored regularly at Arogya Hospital until their bones are fully grown.
Types of growth plate injuries — the Salter-Harris classification
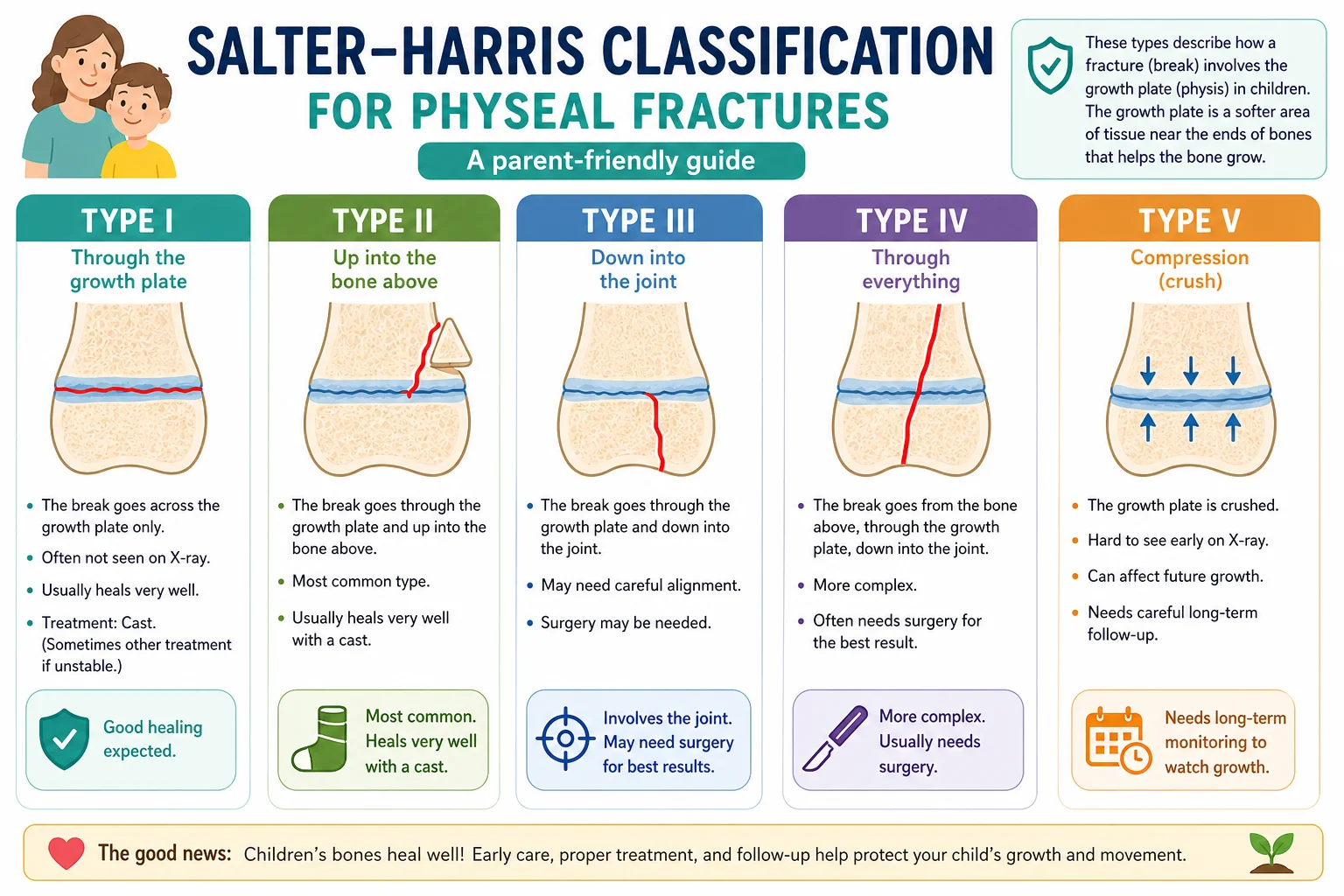
Doctors use a system called the Salter-Harris classification to describe how a fracture relates to the growth plate. There are five types — the higher the number, the more of the growth plate is involved, and the more careful the treatment needs to be.
I. Fracture through the growth plate only
The break passes only through the growth plate, separating the end of the bone from the shaft. The bone itself is intact. These can be hard to see on X-ray and are sometimes diagnosed just from tenderness over the growth plate area.
Outlook: Excellent — growth problems are rare
II. Fracture through the growth plate + a piece of the shaft
The break crosses the growth plate and takes a small triangular chip from the bone shaft along with it. This is the most common type of growth plate fracture.
Outlook: Very good — growth arrest is uncommon

III. Fracture through the growth plate + into the joint
The break crosses the growth plate and extends down through the rounded end of the bone into the joint. Because the joint surface is involved, precise realignment is essential.
Outlook: Requires careful treatment to protect joint and growth plate

IV. Fracture through the shaft, growth plate, and joint
The fracture line passes through the bone shaft, across the growth plate, and into the joint — crossing all three zones. Surgery is almost always needed to restore alignment and stabilise the growth plate.
Outlook: Higher risk of growth disturbance without accurate treatment
V. Crush injury to the growth plate
The growth plate is compressed by a heavy impact rather than broken apart. There may be no visible fracture on initial X-rays. The crushing can damage the cartilage cells responsible for growth.
Outlook: Most serious type — risk of premature growth arrest; sometimes only recognised later
Take-home message
Growth plate injuries are common in active, growing children — but with the right care, the vast majority heal well and go on to have no long-term problems. The key is early, accurate diagnosis and treatment tailored to your child’s specific injury and stage of growth.
What every parent should remember
- Take limb pain seriously in children.
Unlike adults, children’s bones can fracture through the growth plate even after what seems like a minor fall or sports injury. If your child has pain, swelling, or difficulty moving a limb, get it checked. - X-rays alone don’t tell the full story.
Growth plate cartilage is invisible on X-rays. Your doctor may request imaging of the opposite limb for comparison, or an MRI to assess the extent of injury. - Most injuries do not need surgery.
A well-applied cast and careful monitoring is the treatment for the majority of growth plate fractures. Surgery is reserved for cases where precise realignment cannot be achieved any other way. - Long-term follow-up matters.
Growth complications — if they occur at all — may take months or years to become visible. Regular check-ups at Arogya Hospital ensure any changes in your child’s growth pattern are caught and managed early. - Every child is different.
The right treatment depends on the type of fracture, where it is, how much the bone has shifted, and how much growth your child still has ahead. Dr. Ankita Bansal will guide you through a plan that is right for your child specifically.
“A growth plate injury is not just a fracture — it is an injury to a living, growing structure. Our goal at Arogya Hospital is not only to heal the break, but to protect your child’s growth for the long term.”
— Dr. Ankita Bansal, Paediatric Orthopaedics, Arogya Hospital