Few things frighten a parent more than watching their child break a bone. Beyond the immediate pain and distress, the questions come quickly: Will it heal properly? Will the bone go back to normal? Will it affect how they grow? The good news is that children’s bones possess a genuinely remarkable capacity to heal — often faster and more completely than adult bones. Understanding how this process works can go a long way in easing worry and helping you support your child’s recovery.
Why Children’s Bones Heal Differently
Children’s bones are biologically distinct from adult bones in ways that work strongly in their favour after a fracture. The outer layer of a child’s bone, called the periosteum, is thicker, more active, and more richly supplied with blood vessels than in adults. This means the bone’s own repair system is already primed and ready. Additionally, because a child’s skeleton is still actively growing, there is a large pool of cells whose job it is to build new bone — and these cells respond rapidly to injury.
The result is that children typically heal fractures in roughly half the time it takes adults, and their bones retain the ability to gradually correct minor imperfections in shape after healing — a process called remodelling.
How Does a Fracture Actually Heal?
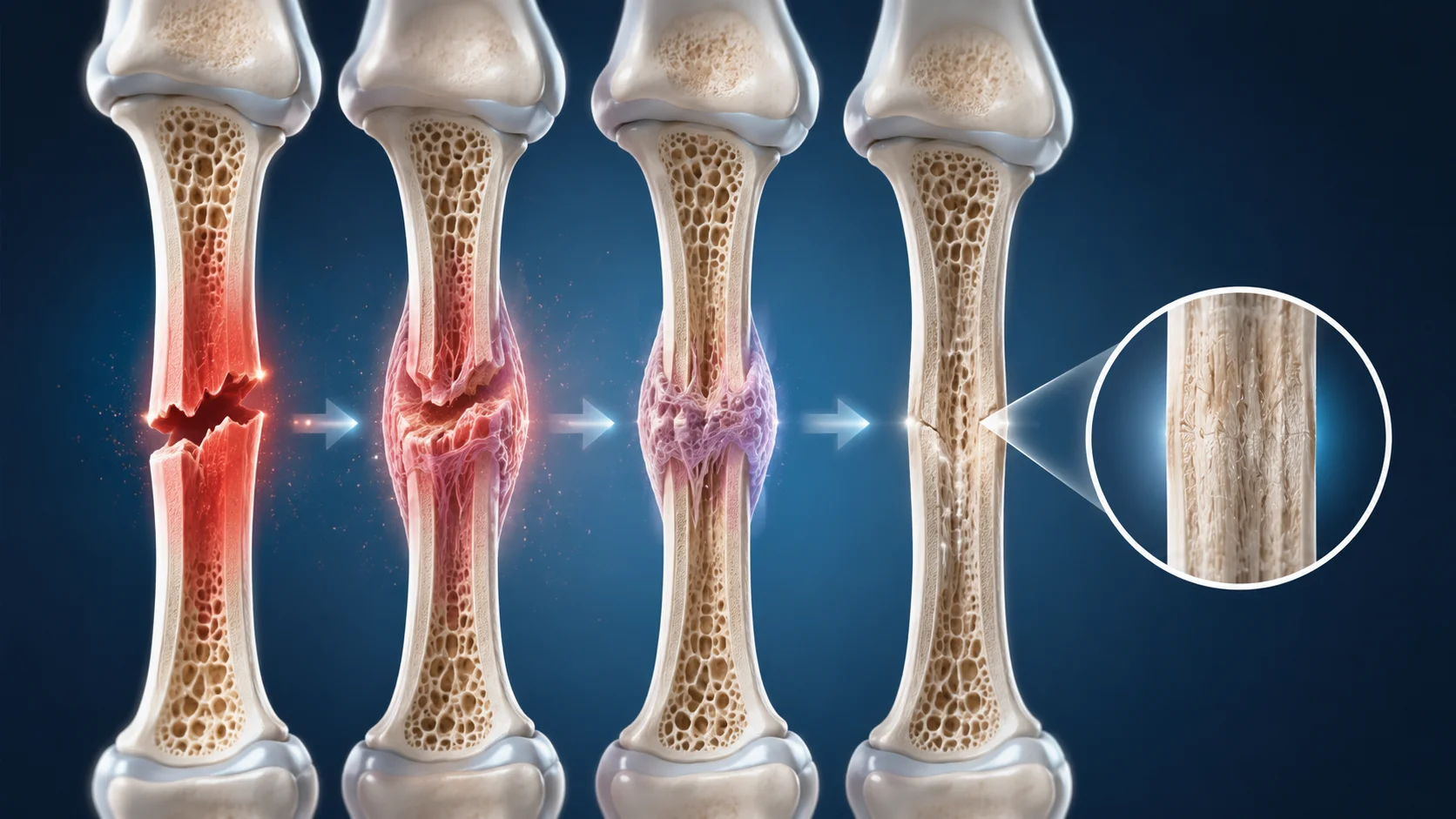
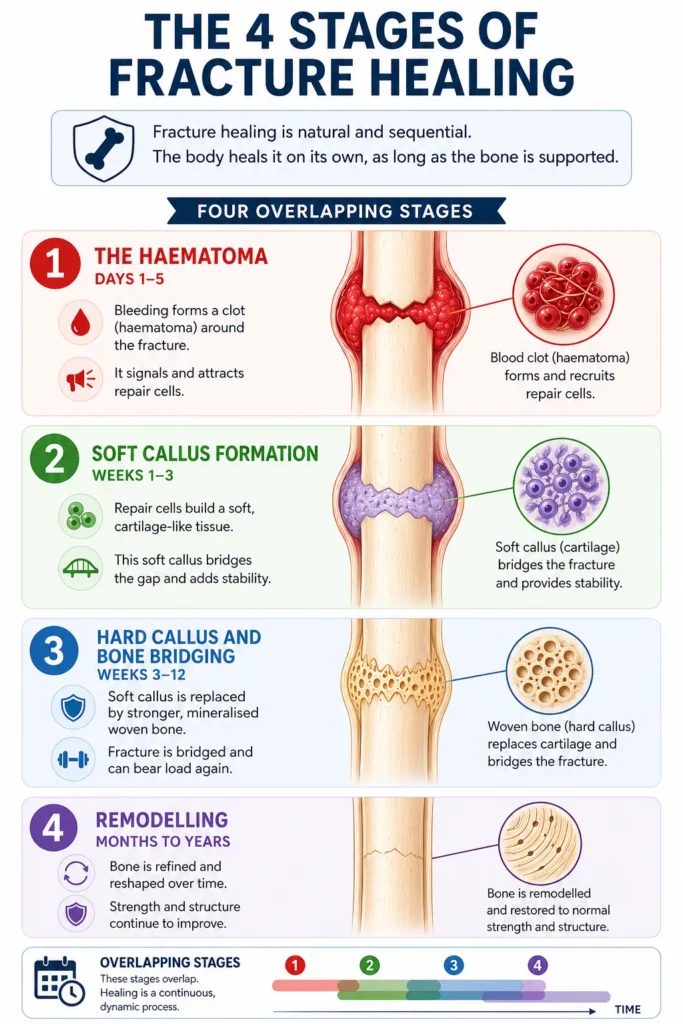
Fracture healing is a natural, sequential biological process. It does not require anything extraordinary — the body manages it on its own, provided the bone is appropriately supported. There are four overlapping stages:
Stage 1 — The Haematoma (Days 1–5)
The moment a bone breaks, small blood vessels in and around the bone are also disrupted. This bleeding forms a clot called a haematoma around the fracture site. Rather than being a problem, this clot is essential — it acts as the scaffold for everything that follows, releasing chemical signals that recruit specialised repair cells to the area.
Stage 2 — Soft Callus Formation (Weeks 1–3)
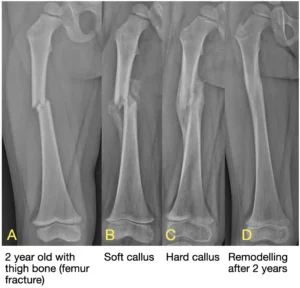
Over the following days to weeks, repair cells called mesenchymal cells arrive at the site and begin multiplying. They first produce a soft, cartilage-like tissue that bridges the gap between the broken bone ends. This is called the soft callus. Though it isn’t bone yet, it provides meaningful stability, and you may notice it as a firm lump under the skin around the fracture — this is entirely normal and a sign that healing is underway.
Stage 3 — Hard Callus and Bone Bridging (Weeks 3–12)
The cartilage callus is progressively replaced by woven bone — harder, stronger, and increasingly mineralised. In children, this callus tends to be thicker and more exuberant than in adults, providing robust support. By the end of this stage, the fracture is typically bridged and the bone can bear load again, though it is not yet at full strength.
Stage 4 — Remodelling (Months to Years)
This final and longest stage is where children have their greatest advantage. The bone continues to be refined and reshaped long after it has clinically healed, as described in detail in the next section.
What Is Bone Remodelling — and How Much Can It Correct?
Remodelling is the process by which the body continues refining the healed bone long after the fracture has united. The bone responds to the mechanical forces placed on it — weight-bearing, muscle pull, and joint movement — and gradually reshapes itself toward a more normal architecture.
This means that even if a fracture heals with some degree of angulation (a slight bend or tilt), a child’s bone may straighten itself over months to years through remodelling. Parents are sometimes shown X-rays at the time of treatment that look imperfect, and this is precisely why — the treating doctor may be confident that remodelling will correct the residual deformity without needing more invasive intervention.
However, remodelling has limits. It works best under specific conditions:
- Age: Younger children have more remodelling potential because they have more growth remaining. A 4-year-old can correct deformities that would be unacceptable in a 12-year-old.
- Proximity to the growth plate: Fractures closer to the ends of bones remodel more effectively than those in the middle of the shaft.
- Direction of angulation: Remodelling works best when the angulation is in the same plane as the nearby joint’s movement. A forward-backward bend near the elbow corrects more readily than a sideways one.
- Degree of deformity: Mild to moderate angulation can remodel; significant displacement or rotation typically cannot, and requires proper correction at the time of treatment.
This is why your child’s orthopaedic surgeon makes individualised decisions about how much correction is needed immediately — it is not a one-size-fits-all calculation.

A Note on Growth Plate Injuries
Some fractures in children involve the growth plate (also called the physis) — the specialised cartilage near the ends of long bones where growth occurs. These injuries deserve special mention because they behave differently from fractures through the shaft of the bone.
Growth plate fractures often heal faster — sometimes within two to four weeks — because of the high cellular activity in that region. This rapid healing is generally beneficial, but it does carry one important implication: any necessary realignment must be done early. Once healing has begun in earnest, attempting to adjust the position of the bone becomes more difficult and risks disrupting the growth plate itself.
The long-term outlook depends heavily on the severity and type of growth plate injury. Fractures that are undisplaced or well-aligned almost always heal without any effect on growth. More severe injuries — particularly those that are significantly displaced or cross through the growth plate — carry a higher risk of growth disturbance, which can manifest as uneven growth or, in rare cases, premature closure of the growth plate. This is why careful follow-up over months — and sometimes years — is recommended after significant growth plate injuries, even once the bone has healed.
For a more detailed discussion, please see our dedicated blog on Growth Plate Injuries.
What Can Slow Down Healing?
While children’s bones heal reliably, a few factors can affect the pace and quality of recovery:
- Nutritional deficiencies: Vitamin D and calcium are essential for bone formation. Children with low levels may heal more slowly.
- Smoking exposure: Even passive smoking has been shown to impair bone healing.
- Fracture displacement: If a fracture shifts significantly from its intended position during healing, further intervention may be needed.
- Underlying health conditions: Conditions such as osteogenesis imperfecta, rickets, or chronic illness can affect the normal healing process.
In otherwise healthy children eating a balanced diet, none of these are typically a concern — but they are worth being aware of.
Key Takeaways for Parents
- Children’s bones heal significantly faster than adult bones, thanks to a thicker, more active periosteum and a robust pool of bone-forming cells.
- Healing progresses through predictable stages: haematoma, soft callus, hard callus, and remodelling — a process that can take months to complete fully.
- The firm lump felt around a healing fracture is the callus. It is a normal, healthy sign of repair.
- Growth plate fractures heal quickly but require early, careful alignment and longer follow-up to monitor for any effect on growth.
- Children’s bones can correct mild post-healing deformities through remodelling — but this capacity depends on age, fracture location, and the degree of deformity.
- Regular follow-up appointments allow your doctor to confirm that healing is progressing correctly and that growth is not being affected.
This blog is part of our series on childhood fractures. For related reading, see our blogs on Types of Fractures in Children, Growth Plate Injuries, and Treatment of Fractures in Children.