
Orthopaedic implants are devices — wires, screws, plates, nails, joint replacements, or external frames — that stabilise or replace bone and joint structures, allowing healing or restoring function.
This article explains the types of implants used in orthopaedic surgery, what they are made of, and when each might be used.
Implant Materials
Most orthopaedic implants are made from stainless steel (316L grade) or titanium. Stainless steel is strong, durable, and cost-effective. Titanium is more expensive but slightly more flexible and very well tolerated by the body, making it preferable for long-term implants such as joint replacements. In most situations, both materials perform equally well for fracture fixation.
Some screws are made from bioabsorbable materials — polymers such as polylactic acid (PLA) or polyglycolic acid (PGA) — that gradually dissolve in the body over months to years. These eliminate the need for a second surgery to remove the implant and are particularly useful in ligament reconstruction, cartilage surgery, and certain paediatric procedures.
Bone cement (polymethylmethacrylate, or PMMA) is not used to make implants but is used alongside them — most commonly in joint replacement surgery — to bond a prosthesis to the surrounding bone.
What Determines the Choice of Implant?
The choice of implant — both its type and its material — is never straightforward and depends on multiple factors working together. The location of the fracture or problem matters enormously: a fracture near a joint requires a different solution to one in the middle of the bone shaft. The type and pattern of the fracture influences whether a nail, plate, or screws will provide the most stable fixation. The age of the patient plays a key role, particularly in children where growth plates must be considered and implant removal is often planned from the outset. Bone quality — whether the bone is normal or weakened by osteoporosis or disease — affects which implant will hold securely. Finally, surgeon experience and preference, local availability of implant systems, and the facilities of the operating centre all contribute to the final decision. There is often more than one correct answer, and the best implant is the one best suited to the individual patient and their circumstances.

Types of Implants
1. K-Wires and Pins
Kirschner wires — K-wires — are thin, smooth stainless steel wires used to hold fractured bone fragments in place while healing occurs. They are one of the most widely used implants in orthopaedic surgery, particularly for fractures of the hand, wrist, and elbow. They can be left protruding above the skin for easy clinic removal, or buried beneath the skin. They are a temporary implant and are removed once healing is sufficient.

2. Screws
Screws are among the most versatile implants in orthopaedic surgery, used alone or combined with plates and other devices. They may be made from stainless steel, titanium, or bioabsorbable polymers, each suited to different situations.
Cortical screws grip the hard outer layer of bone; cancellous screws have a wider thread for the softer bone found at the ends of long bones. Cannulated screws are hollow, allowing them to be guided over a wire for precise placement — particularly useful in hip fractures and other areas where accuracy is critical. Partially threaded screws compress a fracture site together, while fully threaded screws are used where compression is not desired. Headless screws sit flush beneath the bone or cartilage surface, ideal near joints. Interference screws — often bioabsorbable — are used in ligament reconstruction surgery such as ACL repair, securing the graft within the bone tunnel.
Screw size is defined by shaft diameter and is matched carefully to the bone and the clinical situation.

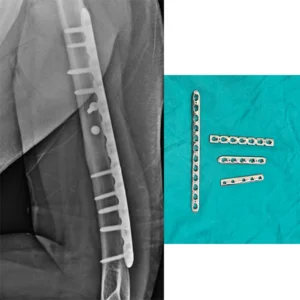
3. Plates
Plates are flat metal structures fixed to the outer surface of bone using screws, acting as an internal splint across a fracture or osteotomy. Standard plates rely on friction between plate and bone; locking plates — now widely used — have screws that lock into the plate at a fixed angle, providing far greater stability. This is especially important in osteoporotic bone or fractures close to joints.
Plates come in a wide range of sizes (commonly 1.5 mm, 2.7 mm, 3.5 mm, and 4.5 mm systems) and many are pre-contoured to fit specific bones. Some specialised plates — such as the Dynamic Hip Screw (DHS) — combine a plate with a large sliding screw and are designed specifically for hip fractures, one of the most common injuries in older adults.

4. Intramedullary Nails
Intramedullary nails are rigid metal rods inserted into the medullary canal — the hollow centre of a long bone — spanning the fracture from within. This makes them particularly effective for fractures of the shaft of the femur (thighbone), tibia (shinbone), and humerus (upper arm). Because the nail lies inside the bone along its mechanical axis, it shares weight-bearing load very effectively, often allowing earlier mobilisation. Locking screws passed through either end of the nail prevent rotation and shortening.


5. Titanium Elastic Nailing System (TENS) — Primarily Used in Children
TENS nails are flexible titanium rods inserted in pairs into the medullary canal, designed specifically for children. Their elasticity creates a three-point fixation without crossing the growth plate, making them well suited to growing bone. They are most commonly used for femur and forearm fractures in school-aged children and are removed once healing is complete.


6. External Fixators
External fixators stabilise bone from outside the body through pins or wires inserted into the bone and connected to a rigid external frame. They are used as temporary stabilisation in severe or open (compound) fractures, or as definitive treatment where infection risk makes internal implants less suitable. Advanced systems such as the Ilizarov ring fixator and computer-guided hexapod frames allow gradual correction of bone length, alignment, or rotation over weeks, without further surgery. They are used in both adults and children.


7. Joint Replacement Implants (Arthroplasty)
When a joint is severely damaged by arthritis, fracture, or other disease, the damaged surfaces can be replaced with artificial components. This is called arthroplasty. Total hip replacement and total knee replacement are among the most commonly performed elective surgical procedures worldwide, with excellent long-term outcomes. Shoulder replacements, elbow replacements, and replacements of smaller joints such as the finger and toe joints are also performed.
Joint replacement implants are typically made of metal alloys (cobalt-chrome or titanium) combined with a polyethylene (plastic) bearing surface. Some designs also incorporate ceramic components. The implant may be fixed to the bone using bone cement (cemented fixation) or designed with a porous surface that bone grows into over time (uncemented or cementless fixation). The choice depends on bone quality, patient age, and activity level.
8. Spinal Implants
A wide range of implants is used specifically in spinal surgery. Pedicle screws are inserted into the vertebrae and connected by metal rods to stabilise the spine after fracture, deformity correction, or spinal fusion. Interbody cages — made of titanium or PEEK (a strong polymer) — are placed between vertebrae to restore disc height and promote fusion. Laminar hooks and sublaminar wires are used in some deformity correction surgeries. Spinal implants are used for conditions ranging from traumatic fractures and scoliosis to degenerative disc disease and spinal tumours.
9. Suture Anchors
Suture anchors are small implants inserted into bone and loaded with sutures to reattach torn soft tissue — tendons or ligaments — back to their bony insertion. They are widely used in shoulder surgery following dislocation or rotator cuff tears, and around the knee and ankle in ligament injuries. They are available in metal, PEEK, and bioabsorbable materials.
10. Cerclage Wires and Cables
Cerclage wires and cables are flexible stainless steel wires or braided cables looped around a bone to hold fragments together. They are most often used to supplement other fixation — for example, securing a large fragment while a plate or nail provides primary stability — and are also commonly used in fractures around existing joint replacement implants (periprosthetic fractures). These wires are also used in Tension band wiring along with k-wires or screws to fix fractures.


Will the Implant Need to Be Removed?
In adults, many implants are left in place permanently once healing is complete, unless they cause pain or other symptoms. Removal is an elective decision made with the surgeon. In children, implants are more frequently removed — particularly those near growth plates — to avoid interfering with normal growth. K-wires and TENS nails are almost always removed after healing. Bioabsorbable implants dissolve on their own and require no removal. The timing and necessity of removal is always discussed individually based on the patient, the implant, and the clinical situation.